

Addendum to 'Want to Know When You Got Cancer?'
Formatting messed up the timeline. I drew it out for you PLUS some history

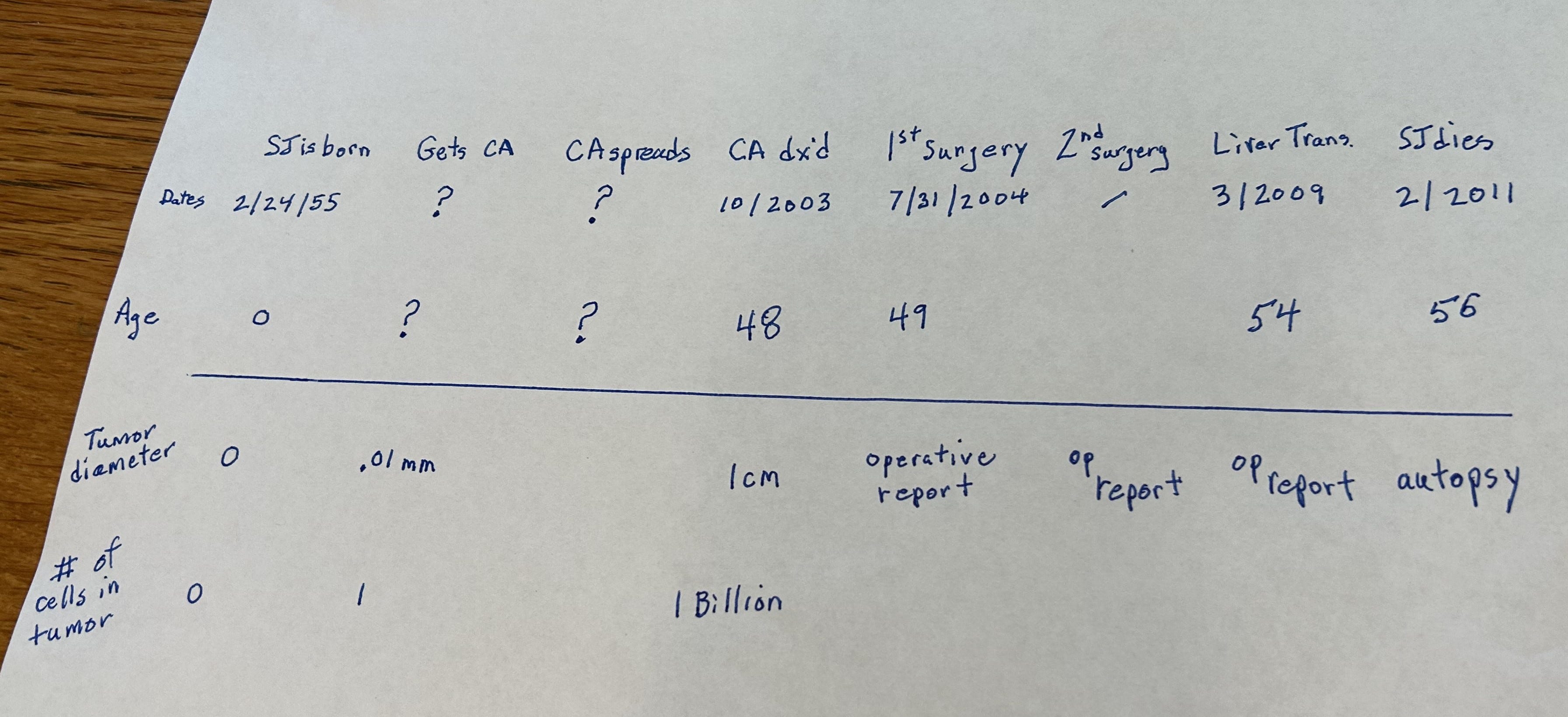
Here is the timeline that got bunched together in the last post:
[Note: In what follows, opening scene dialogue is from the author’s imagination.]
Steve was out driving that fateful evening in October of 2023
”Ouch!”
It was the familiar back pain he had been feeling over the last few years in exactly the same place.
“C’mon, Doc. Just give me a shot of Demerol and let me be on my way." It’s just another kidney stone.”
Except it wasn’t.
… yet another example of a patient jumping to a medical diagnosis when it takes doctors a few blood tests, maybe some radiology and at least an hour, to figure it out…
Ordinarily, Steve would easily be able to convince a young doctor, already in awe and not thinking straight, to do as the billionnaire ordered, but this time it was different.
“No, Mr. Jobs. We need to get a CT. It’ll only take 30 minutes.”
“I just got one! It didn’t show anything!”
(looks through chart) “That was five years ago.”
(mutual stare down)
“If you’d just let me do my job… You’ll be out of here in no time.”
Kudos to this young lady doctor.
The CT didn’t show evidence of kidney stones but it did show a pea-sized something in the pancreas.
‘Pea-sized somethings’ in the pancreas demand immediate attention. The best endoscopist was called in and an ERCP was performed on Steve that night. He wasn’t going anywhere.
E.R.C.P. stands for “Endoscopic, Retrograde, Cholangio-Pancreatography” and that pretty much sums up the skill required to perform one competently. Steve knew he was leaving the room where doctors sew up little cuts and write prescriptions and opening the door into the deadly-serious part of the hospital where nurses mill about with dour looks on their faces and very little eye contact is exchanged, where it’s always a little darker and colder and where you rarely see other patients, where nurses start IVs without asking you how you’re doing today.
Here’s a sketch of what they were dealing with:
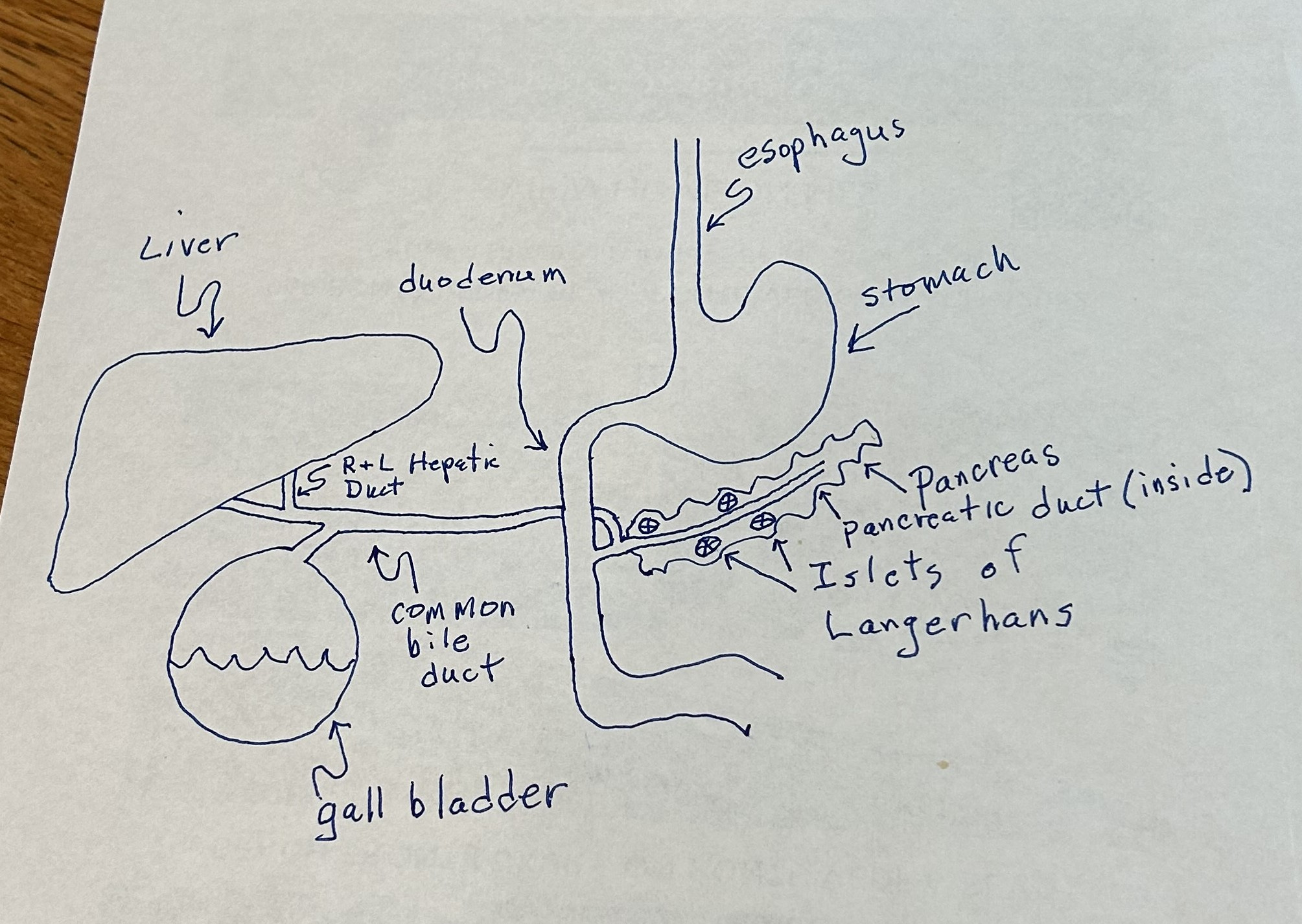
The scope get’s placed through your mouth, down through your stomach and into the duodenum which is the first part of the small intestines. The endoscopist needs to find the little hole in the wall of the duodenum where liver, gall bladder, and exocrine pancreatic secretions empty in. That little hole , the “ papilla at the Ampilla of Vater” is surrounded by a little round sphincter muscle called the “Sphincter of Oddi” that controls when all of those digestive enzymes and emulsifiers can get through. The signal to relax the sphincter being sent from cells lining the duodenum who release hormones into the blood which cause the sphincter to relax and the gall bladder to contract. It’s a tidy system. Eat some fried chicken. The intestine cells have lots of fat from the fried chicken coming into contact with them and release a hormone into the blood which tells the muscular wall of the gall bladder to contract and the sphincter to relax, squirting bile into the small intestine to emulsify those fats.
I wish it looked like that when you get in there to fix something that’s broken. It actually looks like this, given to you as a link because some subscribers may not want to look at it: (click on “Watch on YouTube” to see it)
and, yes, it’s as slippery as it looks…
Fortunately for the endoscopist, he gets to see everything from the inside; the inner lining of the tube that runs through all of us. Yeah, we’re pretty much the same shape as a donut.
In the video that follows, you will see the appearances of the esophagus, stomach and duodenum from the inside. When the endoscopist reaches the duodenum and the voiceover refers to the “papilla” that is where the Ampulla of Vater isThrough which he will enter the pancreatic duct.
He has to go through the little hole and go backwards through the pancreatic duct to get to Steve’s tumor.
Below is a video showing how the ERCP part of the procedure is performed. When they got to the tumor, they sent a biopsy device through one of the ports in the scope and took a piece of it. You have to be very gentle when you do this to make sure you don’t cause pancreatitis. This is where skill is at a premium.
Incidentally, this is how common bile duct stones can sometimes be retrieved. If the endoscopist can’t get the stones out with the ERCP scope, they call someone like me (when I used to do general surgery) to come in- usually at 3 am- and open up the patient. I just go right to it and take it out surgically. It sounds easier than it is. It’s a bloody mess in there. Everything looks the same and you don’t want to open the wrong “tube”.
You can see where the pancreatic duct joins with the common bile duct at the Ampulla of Vater and empties through the Sphincter of Oddi in the blown up picture below:
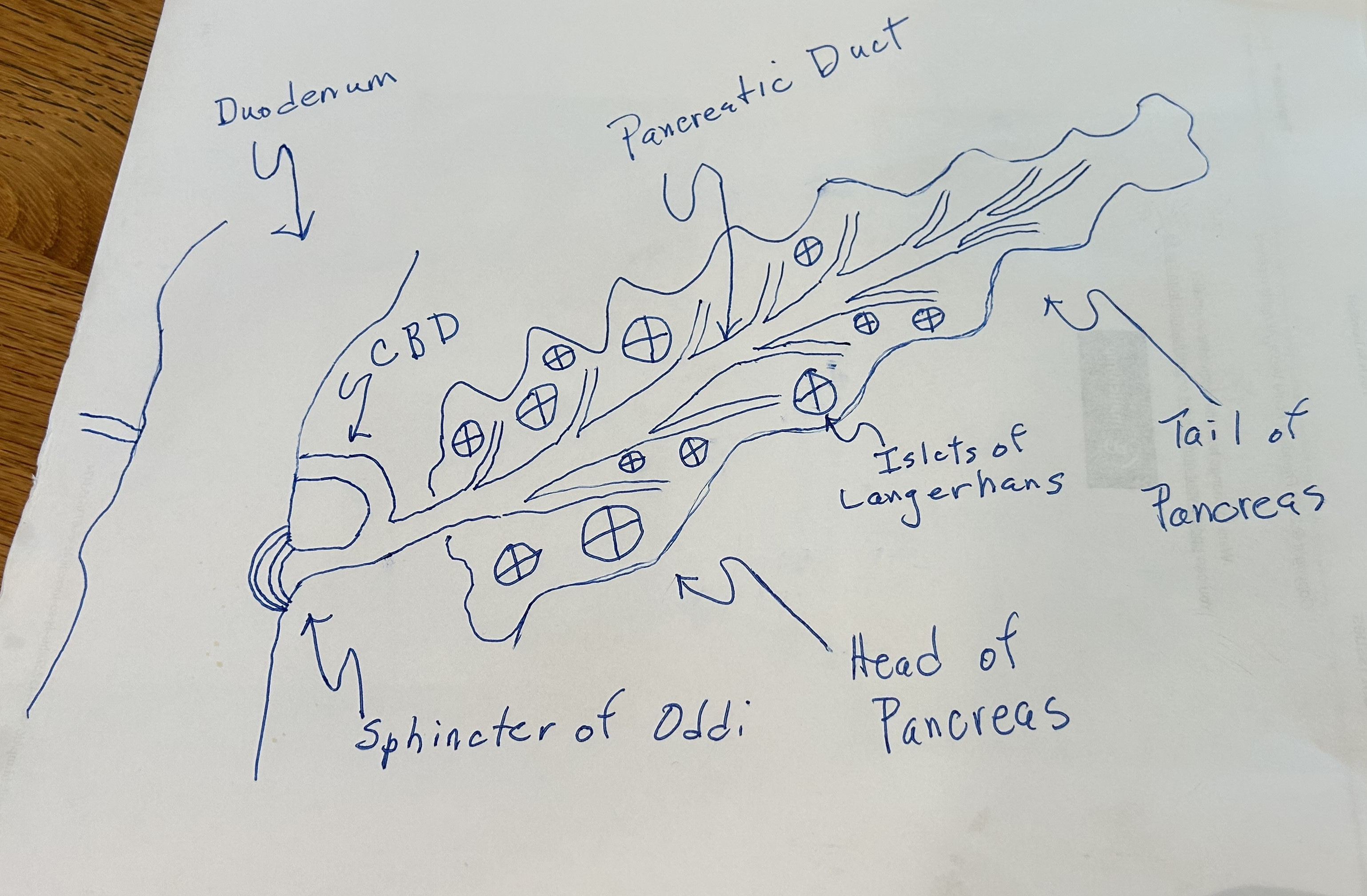
You can also see the Islets of Langerhans there. Islet cells manufacture insulin which, as you know, assists in reducing blood sugar. It is when insulin is inadequate in function (insulin resistance) or amount that diabetes occurs. Typically, people who eat too much sugar, “burn out” their Islet cells and no longer produce the amount of insulin necessary to keep their blood sugar at safe levels. The result is sugar molecules getting deposited everywhere- nerves, lenses, kidneys, etc.- causing water to enter those tissues (due to osmotic pressure), thus damaging them. You can’t see through lenses whose shape has been distorted. Thus the high percentage of patients with diabetes who get cataract operations. Incidentally, insulin is a protein hormone and as such would get eaten up in the stomach if you took it in pill form. Because of this, you have to inject insulin. Bummer. Steroid hormones like estrogen can be taken by mouth because they are derived from cholesterol.
Given that Steve had pancreatic cancer, he was fortunate to have the slower growing variety that arises from Islet cells.
Its the kind that arises from the pancreatic parenchyma- the exocrine part of the pancreas that makes the enzymes that go down the pancreatic duct, that cause the very aggressive cancers where the doctor will usually tell you, sadly, “You have about six months to live”.
Please stop smoking and never start.
The specimen from Steve’s tumor was sent to pathology immediately and the diagnosis came back, “Islet cell cancer of the pancreas”.
It was nine months before Steve opted for surgery during which time and after- for the rest of his life, actually- he endured the thought that he had cut his life short because he didn’t go in for surgery immediately.
All of the people who maintained that position were wrong, of course. His surgeons should have explained all of this to him. Most likely, they didn’t understand it either.
VERY interesting, including the photos, videos and your great diagrams. (Makes me think twice when i eat too much peanut butter). I am wondering, since you are a surgeon, are you seeing more and younger people with various cancers? I just don't remember there being that much cancer 40 to 60 years ago; it seemed realatively rare and was mostly among the elderly. . . now it seems like it's just considered normal, even among the young . . . what do you think?
Fascinating Reid, thanks.